Seems to have worked very well in South Korea! ![]()
"Are you a naturopathic “doctor”? All of those suggestions are gibberish and will only lighten the wallet " (nisser, Canada)
The medical professionals in Switzerland agree with most of Werner’s contributions. He is a medical doctor, and shall be taken seriously, not be made fun of. - Also, if you follow only part of proposals, if will be beneficial.
- May I add, when taking vitamin products, specially vit. A and D, a massive over-dosage should be avoided.
PS: The guy who proposed originally #5, Linus Pauling, had two Nobel Prices, and to my knowledge was not a “naturopathic”.
dombs
I’m also a physician and not a single one of those bullet points has been shown to fight off SARS-cov2. (S)he is welcome to provide evidence to their point though.
Werner gives preventive advice to support the immune system, not a cure. Physicians come in all shapes and colors. Some of them are oriented to prevention and knowledgeable in nutrition, other ones have been brainwashed by an education sponsored by big pharma and try to sell medicine as an exact science. And there’s a continuous spectrum in between. Werner’s bullet points of preventive measures is interesting and most points are supported by nutrition experts (even if his Vit C dosis seems a bit high, Linus Pauling’s claims have been questionned on this point. Anyway it can’t hurt and it’s cheap).
Nisser,
This is a serious question unrelated to how you think about: “Eat fermented food (i.e. Kimchi).”
I wonder what you think about hydroxychloroquine.
As an ophthalmologist I see a lot of patients on this medication (for arthritis and Lupus). It is a very safe medication. I see these patients because they (rarely) develop eye problems after 6 or more years of use. The American Academy of Ophthalmology has said that eye examinations are not required for the shorter periods of use for COVID-19. So not even any rare eye problems to worry about.
There have been some controlled studies in France where viral shedding was reduced.
There is a proposed mechanism: it reduces the expression of the ACE receptor. Any relation to its anti-malarial properties may be coincidental. The COVID-19 virus and Plasmodium falciparum—the most common cause of malaria which is is a unicellular protozoan parasite and not a virus—are very different pathogens.
The virus uses the ACE-2 receptor to enter the cell as you probably already know.
It seems that a pretty good controlled study with thousands of patients could be completed in New York in about 2 weeks (the usually period of the infection).
I live in the US but I do not understand why we do not have an answer on this medication already.
What are your thoughts on this?
Thank you in advance.
Best,
Jim
Furthermore, none of those claims have any substantial proof of doing that. Medicine is based on evidence, not hearsay and tales.
Which leads me nicely into Jrinne’s question.
There’s definitely less enthusiasm in using hydroxychloroquine from our ID colleagues now than early on in the crisis due to very little evidence that it works. I think hey still look at it on a case-by-case basis, particularly if a patient is doing poorly but it is not the standard.
As you know it has quite a number of drug interactions and it can mess with the QT interval. It also seems that a large proportion of COVID patients develop secondary cardiomyopathy so you really want to stay away from throwing more into the mix.
I think here’s a couple of RCTs underway right now so that’ll provide some guidance
My own hunch is that it probably has no bearing on mortality, which is really the only thing that matters right now.
Thank you Nisser.
Jim
There is a big difference between North American medicine and medicine from some other parts of the world. The advice given here is to boost the immune system which is considered a factor in survival. Keep in mind that some view NA medicine as being in the pocket of big pharma. What they are doing is bottling what is readily available in nature and charging a lot of money. I have seen this with my own eyes. My stepson had psoriasis all over his face and body. He had to wait 6 months to see a skin specialist only to be prescribed a steroidal cream which did nothing. My wife, who comes from Russia, then took a specific weed from our backyard, boiled it and put it in her son’s bathwater. The psoriasis started to fade in three treatments and was gone in ten. If big pharma can’t patent a treatment it will never be prescribed.
Just recently my dog who was having neck pain. The vet wanted to do an x-ray, MRI and in the end, perform surgery. Instead, I found a pet chiropractor who corrected my dog’s problem in 15 minutes for a fraction of the cost of what the medical system proposed as the proper way to treat the problem.
I believe that there are a lot of issues with the NA medical system primarily stemming from profits given priority over the patient.
As for Covid-19, I am told that there is one doctor in the south of France that is using hydroxychloroquine exclusively. Apparently treatment has to start early and used in conjunction with antibiotics. He apparently has treated 1524 patients with one death. COVID-19 – IHU
I believe the death was treatment without the anti-biotics but I could be wrong.
Here is a video that warns against hydroxychloroquine with zinc. https://www.youtube.com/watch?v=qmcQMCB2li8&feature=youtu.be
I’m not sure if the doc in France is using zinc or some other form of antibiotic… Someone with medical experience would have to chime in here.
This is why we have trials. He’s welcome to publish his results, get his work critically appraised by his peers and go from there. A website is not the right avenue.
Interesting video.
I remember reading somewhere that there was a contraindication with using chloroquine with azithromycin but then there were also studies using both for malaria. Going by your video it seems that conflict was not resolved. I’ve heard that azithromycin aside from being an antibiotic also has antiviral properties so its ability to treat bacterial pneumonia might not be all the benefit it gives. Chloroquine has both antiviral and immunological properties which explain its use against viral malaria on one hand and also rheumatoid arthritis on the other and why it might help in suppressing both coronavirus and a cytokine storm it might provoke.
Maybe I missed it but did Dr. Roberts say zinc was also contraindicated with chloroquine? Zinc supposedly was able to inhibit reproduction of the original SARS virus and maybe that’s why some doctors include it in a regimen aside from being one of the basic minerals believed to boost the immune system.
His point on FDA approval for chloroquine use for coronavirus is moot at this point. The FDA gave its approval.
That might be my confusion. It has been a few days since I watched the video.
A small study about hydroxychloroquine.
New York Times version: HERE
Original article: HERE
This was a small study. My only comment remains: Why don’t we have a study with 200+ people in New York/New Orleans in about 2 weeks?. Maybe we will.
Actually, I am aware of a study that has enrolled 1,000 healthcare professionals to see if hydroxychloroquine (Plaquinil) can work prophylactically. So, it would be wrong to suggest that the scientific community is sleeping through this.
From the above study:
“…a larger proportion of patients with improved pneumonia in the HCQ treatment group (80.6%, 25 of 32) compared with the control group (54.8%, 17 of 32). Notably, all 4 patients progressed to severe illness that occurred in the control group. However, there were 2 patients with mild adverse reactions in the HCQ treatment group. Significance: Among patients with COVID-19, the use of HCQ could significantly shorten TTCR and promote the absorption of pneumonia.”
Reading studies from doctors can be a frustrating experience. They may have passed medical school but they might fail a writing class. I wonder if other doctors really get the lingo or are just as flummoxed as I am but don’t want to admit it.
Among patients with COVID-19, the use of HCQ could significantly shorten TTCR and promote the absorption of pneumonia.
So no effect on mortality as I suspect. It’s a smalls study and may not be powered enough to see a difference in mortality, you bet they looked at it and likely found it flat, or else they would have commented on it.
It’s a meaningless metric in practice. People aren’t dying from Pneumonias: they’re dying from ARDS, cytokine storm, and cardiac arrest.
Nisser,
Good to see some good use of statistics!
Not only is it a small study, as you say, there is the bias of small studies with any positive result possibly getting published while negative results may not get published.
I just talked to an anesthesia friend who discussed some of the recommendations about EKGs and the risk of prolongation of the QT interval. He started discussing this before I mentioned anything about QT intervals.
Good call on the risks! Some are recommending 12 EKGs before starting hydroxychloroquine, he says.
BTW, my anesthesia friend was quarantining at home (waiting for a negative test). Before he went home he stopped at the hospital pharmacy to fill a hydroxycholoroquine and Z-Pak prescription.
He does not believe in hydroxychloroquine but still he filled the prescription (just interesting).
Best,
Jim
Speaking of cytokine storm, any opinions on CTSO? I’m holding a bit in my coronavirus portfolio.
Walter
Here’s another very grounded answer from an Italian doc. He makes an excellent point.
twitter.com/rob_cosentini/status/1245721133120454662
I don’t have much thoughts on that technology. I don’t see it being used for COVID related storms as they are unpredictable
I wrote up the “cliff notes” of this video.
And this was Dr Roberts’ response:
[quote]
Richard H. Roberts, M.D., Ph.D.:
Your synopsis of my video is very impressive. You hit most or all of the important points in a concise, thorough, and clear manner. You should be a professional writer.
Thanks,
Rich Roberts
[/quote]Dr Roberts himself put out a follow up video where he said that his initial research on zinc is very promising, and although it has not been tested properly yet, in this situation it is not prudent to wait. He himself said that he is taking 15 mg - 30 mg of zinc every day because it wont hurt and may help. Some interesting highlights from this newer video titled zinc coronavirus correlations:[quote]
Lack of zinc causes loss of smell. It also affects ability to fight germs/ immunity. Many older people have zinc deficiency. So they are more at risk of getting COVID-19. This drug opens the cells to allow Zinc to penetrate which inhibits the reproduction of the virus. Zinc also raises the immunity which in turn eliminates much DM II, Hypertension and other conditions, many conditions seen in the elderly.
[/quote]Disclaimer: This synopsis of the new video was not done by me and was not approved by Dr Roberts. It also omits some important disclaimers by Dr Roberts such as that these are correlations; not proof.
This might be an offshoot but it appears that unfortunately when people go on ventilation it appears their chances of survival aren’t that great. Could draw into question the usefulness of manufacturing large quantities of ventilators and how long one can keep someone on a ventilator and still maintain reasonable chances of survival. It’s more anecdotal and of small study numbers mentioned, but still alludes to the concern at hand.
Also studies are showing that Chloroquine is probably ineffective which isn’t surprising. If it was truly a game changer we wouldn’t be still shutting down the economy.
Ubiquitous testing - both for antibodies and active infections is key. Of course a viable vaccine would change the game overnight but everybody is either ready to start of starting trials.
Jeff
Jeff,
Penicillin (an antibacterial) was so effective people could tell immediately that it worked.
Acyclovir (an antiviral) was a game changer but the response is not as impressive as Penicillin and the range of disease is so wide that I do not think we could have been sure that it works without a large controlled study.
Even worse is a medicine like Lipitor. It takes a huge number of people in a controlled study over many years to find its small effect on heart attacks.
I am not going to try to pick a winner as far as a medication. But if the medicine is as effective as, say acyclovir (which would be very good), it will take a pretty large, controlled study, to really show that it works.
Nisser correctly says that a lot of studies are probably “underpowered.” For any medicine we can expect a lot of false positives, selective reporting of positive studies (not the negative ones) and underpowered studies that really tell us nothing.
This is understandable, we will take a little evidence, one way or the other, in this dire situation.
I might ask (you know, write it on a pad) for both hydroxychloroquine and Ganovo+Ritanovir (in Phase IV studies by Ascletis) ) if I were on a ventilator. Can you even write while in the prone position they are now using? It is a dire situation if it is happening to you or a family member. Or just dire period. We are all acting on somewhat educated guesses.
I guess I am just hoping that maybe there is a medicine effective enough that our early underpowered studies are getting us something useful.
I go on about drug company monopolies in another tread. But it is also true that they are the only ones with enough resources to do some of this from beginning to end and it may take some time.
Here is a large list of medications in trial, their target and where they are as far as study phase: Lots of Drugs
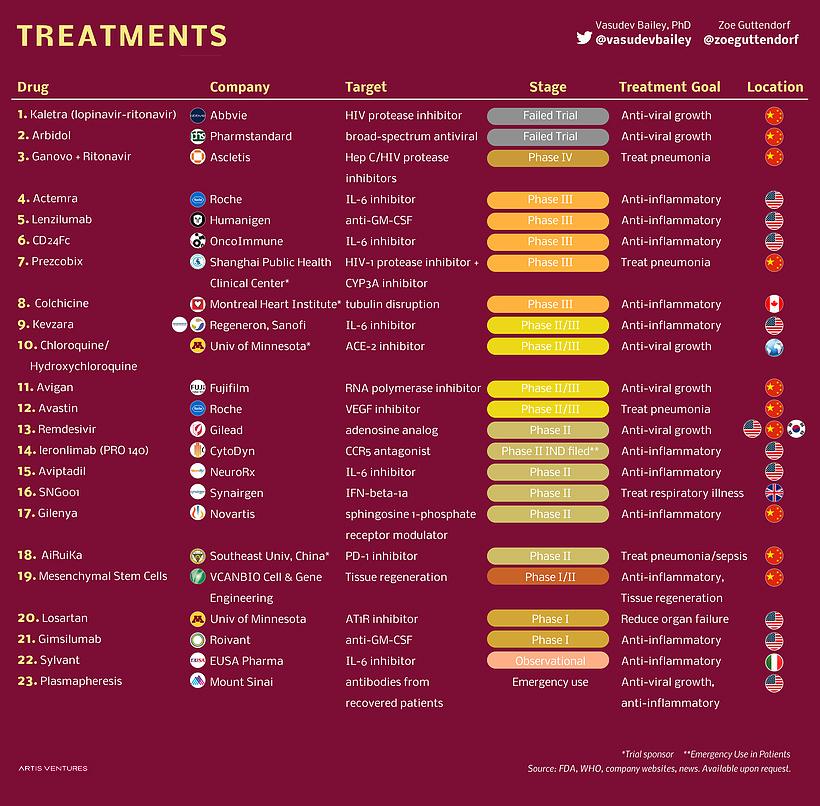{kind=link}
Best,
Jim